As many as two thirds of people with depression do not realize that they have a treatable illness and therefore do not seek professional help. In addition, much of the public, including many health providers, continue to have misperceptions about the disease. The view of depression as a personal weakness or failing that can be willed or wished away leads to painful stigmatization and avoidance of the diagnosis by many of those affected. Do you know what to look for and best practices? Test yourself with our quick quiz.
Which of the following statements about the etiology of depression is true?
A genetic component is nearly always present
Decreased prolactin levels are responsible for depression in children
Major depressive disorder requires a "triggering event"
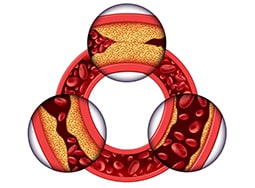
A bidirectional association is noted between depression and coronary artery disease
In older patients, depression is frequently comorbid with chronic medical conditions and can lead to worsening medical outcomes, including mortality. For example, coronary artery disease is a risk factor for the development of depression, and depression is an independent risk factor for the development of coronary disease. Patients with both conditions are more likely to die than those with coronary artery disease alone. Both behavioral and physiologic explanations are likely for these associations. Although some patients have a genetic vulnerability for depression, this is not always present. However, checking for a family history of depression is important.
For more on the etiology of depression, read here.
Which of the following is not recognized as one of the diagnostic criteria of major depressive disorder according to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5)?
Fatigue
Agitation not influenced by external stimuli
Sleep disturbance
Significant weight change
At least five of the following symptoms have to have been present during the same 2-week period (and at least one of the symptoms must be diminished interest/pleasure or depressed mood):
Depressed mood: For children and adolescents, this can also be an irritable mood
Diminished interest or loss of pleasure in almost all activities (anhedonia)
Significant weight change or appetite disturbance: For children, this can be failure to achieve expected weight gain
Sleep disturbance (insomnia or hypersomnia)
Psychomotor agitation or retardation
Fatigue or loss of energy
Feelings of worthlessness
Diminished ability to think or concentrate; indecisiveness
Recurrent thoughts of death, recurrent suicidal ideation without a specific plan, or a suicide attempt or specific plan for committing suicide
Agitation without external stimuli is one of the criteria for diagnosis of depressive episodes with catatonia.
For more on the presentation of major depressive disorder, read here.
Which of the following is necessary for a diagnosis of major depressive disorder with seasonal pattern?
At least four episodes of depressive disturbance in the previous 2 years
Full remission must occur at a characteristic time of year
Seasonal episodes must be at least equal to nonseasonal episodes
Seasonal-related psychosocial stressors must be present
About 70% of depressed people feel worse during the winter and better during the summer. To meet the DSM-5 diagnostic criteria for major depressive disorder with seasonal pattern, depression should be present only at a specific time of year (eg, in the fall or winter), and full remission should occur at a characteristic time of year (eg, spring). An individual should demonstrate at least two episodes of depressive disturbance in the previous 2 years, and seasonal episodes should substantially outnumber nonseasonal episodes. Patients with seasonal affective disorder are more likely to report atypical symptoms, such as hypersomnia, increased appetite, and a craving for carbohydrates.
For more on the presentation of seasonal depression, read here.
Which of the following is indicated if organic brain syndrome or hypopituitarism is included in the differential diagnosis?
MRI or CT scanning
Single-photon PET (SPECT)
PET scanning
Video electroencephalography (video-EEG)
Neuroimaging can help clarify the nature of the neurologic illness that may produce psychiatric symptoms, but these studies are costly and may be of questionable value in patients without discrete neurologic deficits. CT scanning or MRI of the brain should be considered if organic brain syndrome or hypopituitarism is included in the differential diagnosis.
Which of the following statements about the treatment of major depressive disorder is true?
Treatment should be altered if the patient does not have an adequate response to pharmacotherapy in 3-4 weeks
Clinical response to pharmacotherapy is typically seen within 1-2 weeks
Pharmacotherapy is not indicated in patients who have had more than two depressive episodes
Treatment should be continued for 4-9 months in patients with a first episode of major depression not associated with suicidality
Usually, 2-12 weeks at a therapeutic dose, with assumed adherence to the regimen, are needed for a clinical response to become evident. The choice of medication should be guided by anticipated safety and tolerability, which aid in compliance; physician familiarity, which aids in patient education and anticipation of adverse effects; and history of previous treatments. Often, treatment failures are caused by medication noncompliance, inadequate duration of therapy, or inadequate dosing.
According to the 2008 American College of Physicians (ACP) guideline (the most recent release of the guideline) on using second-generation antidepressants to treat depressive disorders, patient preferences should be given serious consideration when choosing the best course of pharmacotherapy for patients with depressive disorders. The patient may want to avoid use of a particular antidepressant if he or she had a previous negative experience with the drug.
The 2008 ACP guideline advises that treatment for major depressive disorder should be altered if the patient does not have an adequate response to pharmacotherapy within 6-8 weeks. Once satisfactory response is achieved, treatment should be continued for 4-9 months in patients with a first episode of major depression that was not associated with significant suicidality or catastrophic outcomes. In those who have had two or more episodes of depression, a longer course of maintenance treatment may prove beneficial. These patients should remain medicated to prevent relapse.
For more on the treatment of depression, read here.